Age/sex: 72-year-old male
Size: 17.0 x 9.8 x 6.4 cm
The specimen shows the lower part of the aorta and the two common iliac arteries (arrows). A small atherosclerotic plaque (A) can be seen in the left one. The aorta is mildly dilated and almost completely occluded by thrombus. At its periphery (P), this has a tan-white appearance with distinct laminations, indicating that it has been present for at least several months. In its central area (C), the thrombus is dark brown and homogeneous, indicating more recent formation (probably hours or days).
Aortoiliac occlusive disease: Leriche syndrome
This is an uncommon condition that is defined classically as a combination of claudication (pain on movement) of the buttocks or thighs, absent or decreased femoral artery pulse, and erectile dysfunction. As demonstrated in this specimen, it is caused by obstruction of the lower aorta and iliac arteries by a combination of atherosclerotic plaque and thrombus. Depending on the rapidity with which the obstruction develops, there may also be findings such as leg muscle atrophy (chronic) and pain at rest (acute). Treatment today involves removal of the thrombus, most often by angioplasty with insertion of a stent through the area of obstruction, or placement of a bypass graft.
Although the condition was first described by Robert Graham in 1826, the eponym associated with it relates to René Leriche, a French surgeon who published the results of his treatment of it in 1940.
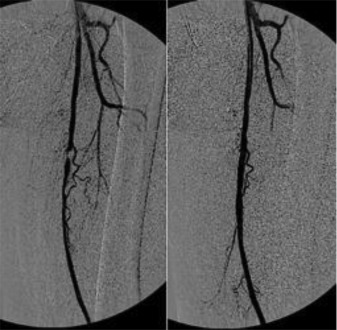
Below: Intraoperative angiography of the superficial femoral artery, before and after stenting.
Source: Figure 1. Intraoperative angiography of the left femoral artery. From “Abnormally high failure rate for femoral angioplasty in patients with pseudoxanthoma elasticum,” by M Ammi, G Kranenburg, L Omarjee, et al. (2015). J Vasc Surg, 1(4), 276-278.