Abbott Specimen 76

Specimen Card Nomenclature
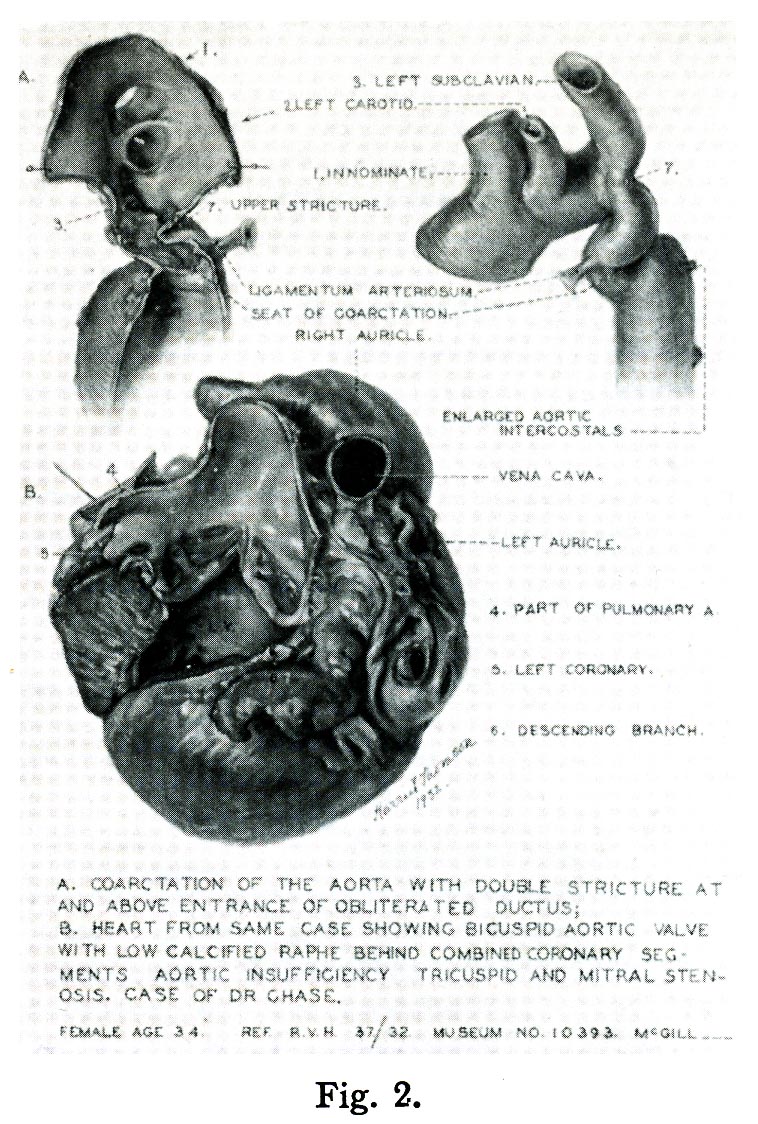
Coarctation of aorta. Mitral stenosis, tricuspid stenosis, and bicuspid aortic
International Classification of Diseases
Coarctation of aorta
Donor
W. H. Chase (Royal Victoria Hospital)
Date
1932
Age
Thirty-four years
Description
The specimen shows part of the aortic arch and the entire descending aorta. A region of marked stenosis (long arrows) can be seen just distal to the left subclavian artery. A portion of an obliterated ductus arteriosus (D) is present at the bottom of the stenotic area. The aorta distal to this is mildly dilated and shows the dilated origin of an intercostal artery (short arrow) that provided collateral blood flow to the descending aorta.
Comment
Aortic coarctation occurs in about 1 to 3 per 10,000 births. The cause is uncertain. Classically, the stenosis may be located proximal or distal to the insertion of the ductus arteriosus. In pre-ductal cases, blood flows to the lower body via a persistent patent ductus. Because other cardiovascular abnormalities are frequently present, this form usually becomes evident at birth or in early infancy.
In post-ductal cases, blood flows to the lower body by an enlarged collateral circulation originating in the proximal aorta and coursing through the mammary and intercostal arteries. Depending on the severity of the stenosis, symptoms may not become evident until adulthood.
This patient had signs of cardiac failure during pregnancy but delivered a healthy baby by C-section at 8 months. She died “quietly in her sleep” 6 days later. As indicated in the card description, she also had valvular disease, including a bicuspid aortic valve; the heart itself has not been kept but is illustrated in the Atlas image.

Atlas Illustration
Plate VIII Figure 2